HRD tests should include a tumour BRCA test, which cannot currently distinguish between germline and somatic mutations. Therefore, if a BRCA mutation is identified, patients will need further genetic tests to identify whether other members of their family are at risk.1,2 Patients should be referred to a genetic counsellor for germline testing who will discuss the potential implications of this test and next steps.
Germline mutation3
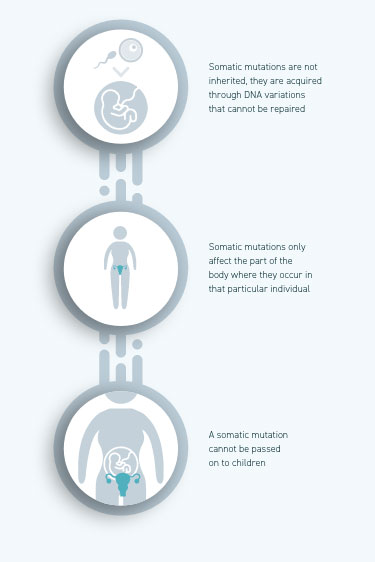
Somatic mutation3
Colour indicates the presence of cells with mutation
Colour indicates the presence of cells with mutation
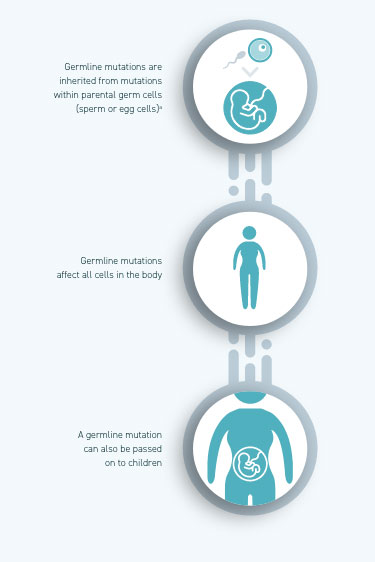
aBRCA mutations can be inherited from either the mother or the father
Colour indicates the presence of cells with mutation
aBRCA mutations can be inherited from either the mother or the father
Role of genetic counsellors
HRD testing can identify patients that are at higher risk of carrying a germline genetic mutation that can have implications for their family. For this reason, it is important to consider the role of genetic counselling. Usually, this is considered after the results of an HRD test are known; genetic counselling is offered to patients with a known BRCA mutation or a strong family history of cancer. Patients who were identified to not have a BRCA mutation, but were still HRD-positive (due to genomic instability), may not need to be referred for genetic counselling.
Genetic counsellors work directly with patients and families, offering genetic/genomic information and support. They are trained to present complex and difficult-to-comprehend information about genetic risks, testing and diagnosis to families and patients4
In terms of HRD, a genetic counsellor will usually become part of the healthcare team once a BRCA mutation has been identified in a patient4
- They will provide information about further genetic testing and related procedures, and can help families understand the significance of genetic conditions or whether there is a strong family history of relevant cancers4
- Mutations that are purely somatic and not found in the germline DNA do not warrant further genetic counselling5
Streamlining counselling methods via telephone and virtual consultations
Genetic counselling can be effectively and efficiently delivered via the telephone/virtually to increase access and decrease costs6–8
provision of written and
digital information
testing
is offered after the test to report
results and offer advice
Please refer to local regulations around testing procedures and requirements
1. Myriad Genetic Laboratories, Inc. myChoice® CDx Technical Information. Available at: https://myriad-web.s3.amazonaws.com/myChoiceCDx/downloads/myChoiceCDxTech.pdf (Accessed July, 2021); 2. Foundation Medicine, Inc. FoundationFocus™ CDxBRCA LOH Technical Information Summary. Available at: https://www.accessdata.fda.gov/cdrh_docs/pdf16/P160018S001c.pdf (Accessed July, 2021); 3. Government of New South Wales Centre for Genetics Education. Variations in the genetic code. Available at: https://www.genetics.edu.au/publications-and-resources/facts-sheets/fact-sheet-2-variations-in-the-genetic-code (Accessed July, 2021); 4. Genetic Alliance; The New York-Mid-Atlantic Consortium for Genetic and Newborn Screening Services. Genetic Counseling. In: Understanding Genetics: A New York, Mid-Atlantic Guide for Patients and Health Professionals. Washington, DC, USA: Genetic Alliance; 2009; 5. Frey MK, Porthuri B. Gynecol Oncol Res Pract 2017;4:4; 6. Hoogerbrugge N, Jongmans MCJ. Eur J Hum Genet 2016;24:S19–S26; 7. Schwartz M, et al. J Clin Oncol 2014;32:618–626; 8. Sie A, et al, BMC Women’s Health 2012;12:12